
Blood Lead Levels in Children Aged 1–5 Years — United States, 1999–2010
Morbidity and Mortality Weekly Report (MMWR)
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Blood Lead Levels in Children Aged 1–5 Years — United States, 1999–2010
Weekly
April 5, 2013 / 62(13);245-248
The adverse health effects of lead exposure in children are well described and include intellectual and behavioral deficits, making lead exposure an important public health problem (1). No safe blood lead level (BLL) in children has been identified. To estimate the number of children aged 1–5 years in the United States at risk for adverse health effects from lead exposure and to assess the impact of prevention efforts, CDC analyzed data from the National Health and Nutrition Examination Survey (NHANES) from the periods 1999–2002 to 2007–2010. This report summarizes the results of that analysis, which indicated that the percentage of children aged 1–5 years with BLLs at or above the upper reference interval value of 5 µg/dL calculated using the 2007–2010 NHANES cycle was 2.6%. Thus, an estimated 535,000 U.S. children aged 1–5 years had BLLs ≥5 µg/dL based on the U.S. Census Bureau 2010 count of the number of children in this age group. Despite progress in reducing BLLs among children in this age group overall, differences between the mean BLLs of different racial/ethnic and income groups persist, and work remains to be done to reach the Healthy People 2020 objective of reducing mean BLLs for all children in the United States (EH-8.2) (2).
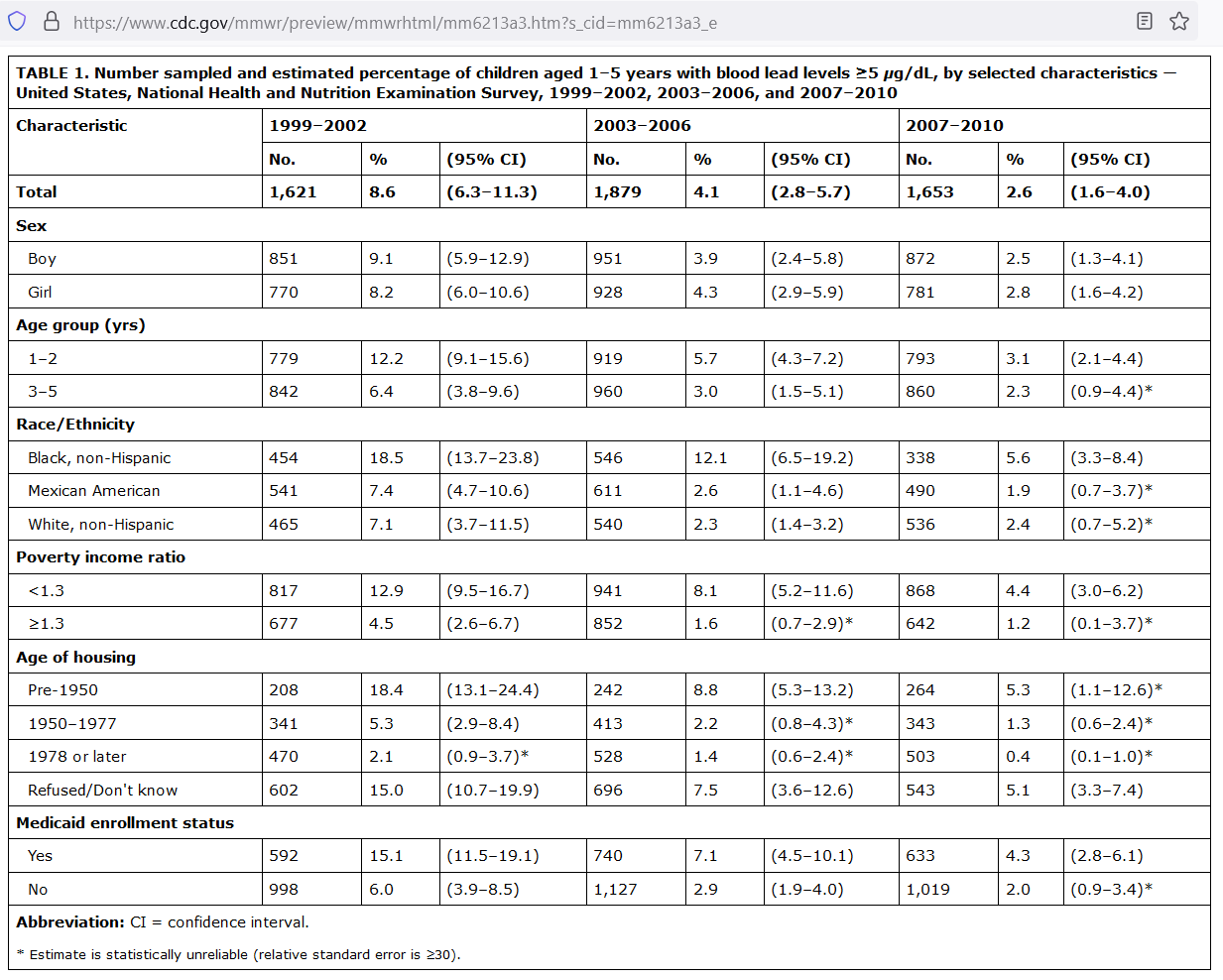
In 1991, CDC defined BLLs ≥10 µg/dL as the "level of concern" for children aged 1–5 years (3). However, in May 2012, CDC accepted the recommendations of its Advisory Committee on Childhood Lead Poisoning Prevention (ACCLPP) that the term "level of concern" be replaced with an upper reference interval value defined as the 97.5th percentile of BLLs in U.S. children aged 1–5 years from two consecutive cycles of NHANES (4). CDC conducts NHANES, a continuous, cross-sectional, representative survey of the noninstitutionalized U.S. civilian population, using a complex, multistage probability design. Since the mid-1970s, when NHANES first began measuring blood lead levels, the survey has become the basis for monitoring changes in BLLs in the United States. Beginning in 1999, NHANES became a continuous survey, with roughly 10,000 NHANES participants interviewed and examined during each 2-year cycle. Approximately 1,240 children aged 1–5 years are examined every cycle, and a blood specimen is drawn from approximately 850 (69%) of them. In NHANES, BLL is measured using inductively coupled plasma mass spectrometry in the elemental analysis laboratory at CDC (5). The current upper reference interval value of the 97.5th percentile of the distribution of the combined 2007–2008 and 2009–2010 cycles of NHANES was calculated as 5 µg/dL.
For this analysis, a BLL ≥5 µg/dL is defined as a high BLL. The geometric mean (GM) BLLs for children aged 1–5 years and 95% confidence intervals (CIs) also were calculated. Data are presented in 4-year aggregates from the 1999–2002, 2003–2006, and 2007–2010 NHANES cycles. Significant differences in GM between categories in selected characteristics were tested using pairwise t-tests. Values below the BLL limit of detection were replaced with the limit of detection divided by the square root of 2, and all data analyses included sample weights to account for unequal probabilities of selection, oversampling, and survey nonresponse (6).
This analysis was focused on demographic categories with long-standing disparities in risk for high BLLs between groups: age, sex, race/ethnicity, age of housing, poverty income ratio (PIR), and Medicaid enrollment status. Race/ethnicity was categorized as non-Hispanic white, non-Hispanic black, Mexican American, and "other." Although children whose race/ethnicity was categorized as "other" were included in overall estimates, they were excluded from estimates stratified by race/ethnicity because of small numbers. PIR was calculated by dividing the total annual family income by the federal poverty threshold specific to family size, year, and state of residence. PIR was categorized as either <1.3 or ≥1.3 times the poverty level.
In bivariate analyses, the CI for the 2007–2010 NHANES estimates of the percentage of non-Hispanic black children (3.3%–8.4%) and non-Hispanic white children (0.7%–5.2%) with BLLs ≥5 µg/dL overlap (Table 1). However, disparities in the GM BLL by factors such as race/ethnicity and income level, which have been important historically, persist. The difference between the GM BLL of non-Hispanic black children (1.8 µg/dL [CI = 1.6–1.9]) GM BLL compared with either non-Hispanic white (1.3 µg/dL [CI = 1.1–1.4]) or Mexican American (1.3 µg/dL [CI = 1.2–1.4]) children remains significant (p<0.01) (Table 2). The difference in GM BLL among children belonging to families with a PIR <1.3 compared with families with a PIR ≥1.3 also is significant (1.6 µg/dL versus 1.2 µg/dL, respectively [p<0.01]), as is the difference in GM BLL by age group and Medicaid enrollment status (Table 2).
https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6213a3.htm?s_cid=mm6213a3_e
Comments